
Christian Sex Therapy
with a 93.6% success rate!
 Get Started
Get StartedWhy do women lose their sexual desire? More importantly: What can you do about low sexual desire? In this article, we take a look at the ways female sexual desire is different than male sex drive. If we don’t understand how wives are unique, our attempts at understanding the loss of libido will be…well…frustrated.
- Parts of this article were written by Rick Reynolds, LCSW and appeared first as Recovering from infidelity: Difficulties with Intimacy
Wives sexual desire is a subject misunderstood by nearly all men and most women.
In recent years, one of the hottest topics in sexology has been female sexual desire disorders. For the past four decades, women have been pathologized for not being like men. For instance, according to University of British Columbia psychiatrist Rosemary Basson, “sexual difficulties are particularly prevalent among women seeking routine gynecological care.2 In population surveys, some 30%–35% of women aged 18–70 have reported a lack of sexual desire during the previous 1–12 months.3,4”
The traditional assumption for both men and women has been that desire precedes sexual arousal. Therefore, if a woman is no longer experiencing desire, it is assumed that she now has some sort of sexual hang-up or disorder. While this may be true for men, research in the past 10 years reveals a different pattern for women.
Men tend to be more like a loaded gun ready to fire. All that’s needed is someone to pull on the trigger. A man’s libido acts as a drive similar to hunger or thirst. For the past hundred years, sex professionals have assumed that a woman’s libido was at least similar and that if a woman didn’t feel desire something had to be wrong.
Contributing to the problem are the messages delivered through media. Women are sexually portrayed in books, movies, articles, and even in church circles as men in female form. This mistaken belief concerning female arousal and response patterns has left generations of men and women believing something that’s false. Hardly a day goes by that some couple doesn’t come into my office arguing about the wife’s lack of sexual desire. This leaves women feeling that they are somehow flawed because they don’t share the same sexual interest as their husband.
But what if desire does not precede arousal?
That is exactly what Basson discovered after interviewing hundreds of women. Contrary to the conventional model, for many women desire is not the cause of lovemaking, but rather the result. Basson’s research revealed that women often begin sexual experiences feeling sexually neutral. But as things heat up, so do they – and eventually, desire is experienced.
This explains why Viagra doesn’t work for women, and why sex-boosting supplements are only minimally successful. Products that change the physiology of sexual arousal do not affect desire. At best, they can only increase blood flow to the genitals. It’s easy for men to be aware of increased blood flow because erections are hard to miss. From there it’s only a short step in a man’s mind from erection to the assumption that they have desire. Women, on the other hand, are often unaware of gentle blood engorgement, and even when they are aware of it they frequently report no feelings of arousal.
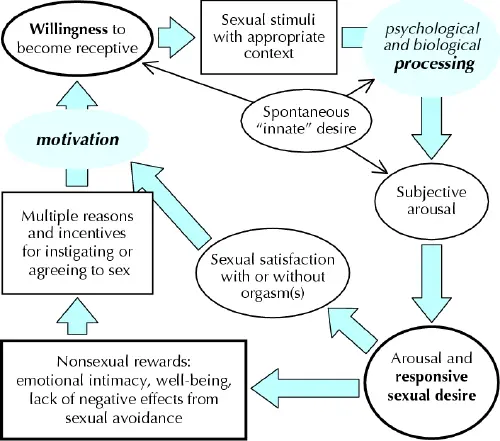
Click for Fig. 1: Sex response cycle, showing responsive desire experienced during the sexual experience as well as variable initial (spontaneous) desire. At the “initial” stage (left) there is sexual neutrality, but with positive motivation. A woman’s reasons for instigating or agreeing to sex include a desire to express love, to receive and share physical pleasure, to feel emotionally closer, to please the partner and to increase her own well-being. This leads to a willingness to find and consciously focus on sexual stimuli. These stimuli are processed in the mind, influenced by biological and psychological factors. The resulting state is one of subjective sexual arousal. Continued stimulation allows sexual excitement and pleasure to become more intense, triggering desire for sex itself: sexual desire, absent initially, is now present. Sexual satisfaction, with or without orgasm, results when the stimulation continues sufficiently long and the woman can stay focused, enjoys the sensation of sexual arousal and is free from any negative outcome such as pain. (Modified from Basson 2001,14 and published with the permission of the American College of Obstetricians and Gynecologists.)
If women don’t experience a sense of desire, as most men know it, then most guys might wonder why a woman would even want to be sexual. According to research, women tend to be sexual for reasons that affirm their relationships, but their reasons are not inherently sexual. These might include wanting to please their lover, a desire to feel close, to prevent strife, to reconnect after a fight, or because they feel a responsibility. Research supports the old adage that men become intimate to have sex and women have sex to become intimate.
“The critical question becomes not how do you ignite a woman’s desire for sex, but instead, what kind of interaction arouses women sufficiently to enable them to experience desire?”
The types of interaction that fuel desires in women are playful, leisurely, sensual (lovemaking based on whole body massage that can include genitals but certainly is not focused on them). In surveys, the primary complaints of women are about interactions with their husbands which are non-sensual, too rushed, too focused on breasts and genitals, and too quickly plunged into intercourse. Rushed lovemaking fails to give women the time most need to respond to become aroused enough to experience desire.
Further complicating the issue is the culture created by Viagra. Men mistakenly believe they are sexually aroused when they have an erection. Therefore taking Viagra and having an erection means they’re good to go. However, erections have nothing to do with psychological arousal. Any erectile medication can give a physical erection, but does it create an excitement to be with your mate and to experience the wonder of who they are? Far too often a man’s genitals on Viagra will be at 100%, but his psychological arousal remains at 10 or 20 percent. Once the erection is in place, he proceeds on to intercourse, skipping the steps which would create psychological arousal for both himself and his wife. This creates a growing sense of dissatisfaction for the woman since she is not experiencing the necessary relational interactions and arousal to make the experience pleasurable for her.
Research shows that many women do experience spontaneous desire and interest when they’re involved in a new relationship or when coming back together after long-term separation from their partner, but it also indicates that most women in long-term relationships rarely think about sex or experience spontaneous sexual desire. Therefore, women seem to operate more out of a point of sexual neutrality–where she is receptive to being sexual but does not initiate sexual activity. Many women report that the goal of sexual activity is not necessarily orgasm but rather personal satisfaction, which is then experienced as physical satisfaction (orgasm) and/or emotional satisfaction (the feeling of closeness and connection with a partner).
“There is not something necessarily wrong if a woman is not experiencing the same desire and arousal patterns as a man. Men and women are not the same.”
Women need to quit being so hard on themselves if they don’t experience the same desire as their husbands. And men need to quit thinking there must be something wrong with their wife if she doesn’t experience sexual desire as he does.
If men or women experience a lack of desire in a marital relationship. Multiple factors need to be explored: The following is a list of factors from Rosemary Basson’s article.
Women’s Sexual Dysfunction: Revised and Expanded Definitions
Interpersonal and contextual factors
In a recent national probability sample of American women 20–65 years of age, their emotional relationship with the partner during sexual activity and general emotional well-being were the 2 strongest predictors of absence of distress about sex. Women who defined themselves (using standard psychological instruments) to be in good mental health were much less likely than women with lower self-rated mental health to report distress about their sexual relationship (odds ratio 0.41, 95% confidence interval 0.29– 0.59). The healthier women were therefore 59% less likely to report distress about their sexual relationship. Feeling emotionally close to their partner during sexual activity decreased the odds of “slight distress” by 33% relative to “no distress,” and “marked distress” by 43%; in other words, the stronger the emotional intimacy with the partner, the less distress.Other contextual factors reported to reduce arousability included concerns about safety (risks of unwanted pregnancy and STDs, for example, or emotional or physical safety), appropriateness or privacy, or simply that the situation is insufficiently erotic, too hurried, or too late in the day.
Personal psychological factors
Frequently a woman’s arousal is precluded by the nonsexual distractions of daily life, but also sometimes by sexual distractions (e.g., worry about not becoming sufficiently aroused, reaching orgasm, a male partner’s delayed or premature ejaculation or a female partner’s lack of orgasm). Empirical studies have shown a high correlation of desire complaints with measures of low self-image, mood instability and the tendency toward worry and anxiety (without meeting the clinical definition of a mood disorder). Differences between a group of 46 consecutive women with a diagnosis of desire disorder without clinical depression and a control group of 100 healthy women were significant for 6 out of 8 scales in the Narcissism Inventory (a standardized self-administered instrument). The scales indicated that the women with desire disorder had self-esteem that was weak or even fragile, emotional instability, anxiety, and neuroticism. Sexual arousal and orgasm, especially in a partner’s presence, necessitates a certain degree of vulnerability, which is impossible for some women who cannot tolerate feelings of loss of control generally, and loss of control specifically of their body’s reactions.
Further inhibiting psychological factors include memories of past negative sexual experiences, including those that have been coercive or abusive, and expectations of negative outcomes to the sexual experience (e.g., from dyspareunia or partner sexual dysfunction).
Biological factors
The biological and pathophysiological underpinnings of normal and abnormal female sexual response are only recently receiving attention. Most of the basic science and animal experiments in this area are beyond the scope of this review. Some promising attempts are noted, however, in part because they relate attempts to ameliorate sexual dysfunction by means of off-label use of available drugs and to avoid the negative sexual side-effects of medications such as antidepressants.
Depression is strongly associated with reduced sexual function. Of 79 women with major depression surveyed before treatment with medication, 50% reported decreased sex drive; 50%, more difficulty obtaining vaginal lubrication; and 50%, far less sexual arousal when engaging in sex. Only 50% had been sexually active during the previous month. In addition, sexual dysfunction can constitute an adverse event of antidepressant use, especially among patients who had low levels of sexual enjoyment before the onset of their depression. When patients are specifically asked about sexual side-effects, they are acknowledged by as many as 70%.
Sexual dysfunction is also a common side-effect of treatment with antidepressants. Among women being treated, it has been found to be more common in those who are older, married, without postsecondary education, without full-time work, or taking concomitant medication (any type); those who have a comorbid illness that might affect sexual functioning, or a history of antidepressant-associated sexual dysfunction; those who deem sexual function unimportant; and those whose previous sexual engagements had afforded little pleasure.
Currently under scrutiny is the role of dopamine and other neurotransmitters in influencing sex hormone receptors and how the neurotransmitters are, in turn, influenced by sex hormones. Estrogenized female animals change their sexual behavior when administered progesterone; studies have shown that the same changes can result from dopamine or the presence of a male animal. Among 75 non-depressed women with a DSM-IV diagnosis of hypoactive sexual desire disorder who received bupropion (a dopaminergic drug; average dose 389 mg/ d) or placebo, improvements in pleasure, arousal and orgasm were statistically significant for those administered the active drug. Interestingly, these changes were unaccompanied by increased desire.
Testosterone itself is being investigated as to its role in sexual function and dysfunction. About half of daily testosterone production in women is from the ovary. Some women with sudden loss of all ovarian production of androgens lose their sexual arousability. Supplementation to high physiological (as opposed to pharmacologically evident) levels of testosterone recently have led to increased arousability and more intense orgasmic experiences, but not to increased sexual thinking, fantasizing or spontaneous desire. Of 75 surgically menopausal women aged 31–56 participating in a randomized clinical trial of testosterone versus placebo, those given testosterone (300 μg transdermally) in addition to estrogen reported increased frequency of sexual activity, sexual pleasure and intensity of orgasm. So, reminiscent of the animal model, supplementation with a dopaminergic drug or testosterone can increase some women’s sexual arousability; but so too, as in the animal model, can environmental change (a new partner).




{kind=link}